Introduction: Each year, thousands of patients suffer from sacral decubitus ulcers, also known as pressure ulcers or sores. The current standard of care for sacral decubitus ulcer treatment is expensive and suboptimal, ranging in cost from a 15-dollar tube of Neosporin Ointment to 240,000 dollars for a skin flap surgery. Grade II pressure sores inevitably progress to stage III and IV if not addressed aggressively and early. Late-stage pressure sores present a unique challenge to physicians, particularly when they are deep, tunneling, and have tendon or bone involvement, as is the case for the two patients in this case study.
The first patient in this study (referred to as patient 1) was afflicted with a mid-sacral pressure sore with exposed tendon, bone, and tunneling of ten years duration. The second patient in this study (referred to as patient 2) suffered from an ischial pressure sore with exposed tendon, bone, and tunneling for 30 months.
Methods: Both patients exhausted conservative measures, including wound vac placement, oral and IV antibiotic treatment, multiple episodes of sharp debridement, wet-to-dry dressings, silver sulfadiazine dressings, and dehydrated amniotic membrane allograft placements. After failing conservative management, both patients received several applications of Wharton’s Jelly, a mesenchymal connective tissue allograft, to accelerate wound closure. Conservative management, including sharp debridement when necessary, oral antibiotics, and electrical stimulation, were used in conjunction with the WJ allograft applications.
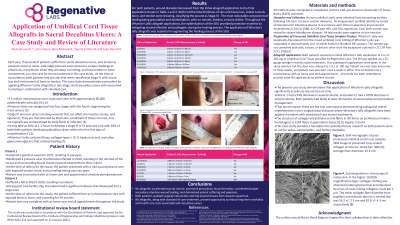
Results: At the time of consultation with Dr. Michael Lavor, both patients’ wounds were classified as Stage IV with tissue loss and involvement of bone or tendon, according to the National Pressure Ulcer Advisory Panel (NPUAP). After eight months of standardized wound care treatment combined with multiple Wharton’s Jelly applications, a mesenchymal connective tissue, both patients had wounds showing over 90% contraction in depth, tunneling, and diameter.
Discussion: This case study demonstrates a precedent for applying Wharton’s Jelly, a mesenchymal connective tissue (MCT), allografts in late-stage sacral decubitus ulcers with associated tunneling in combination with standard of care to promulgate wound closure from deep to superficial, promote an environment for granulation tissue to form, and ultimately create a more suitable environment for dehydrated amniotic membrane allograft application. Future research efforts may be directed at the frequency, concentration, and procedural techniques that best promote granulation tissue formation and volumetric contracture of deep wounds by secondary intention from the bottom up.

.png)