(CR-027) Lights, Fluorescence, Action (against bacterial load): Assessment and treatment decisions of 1000 wounds across 211 U.S. facilities
Friday, April 28, 2023
7:15 PM - 8:30 PM East Coast USA Time
Laura Jones, PhD – MolecuLight, Inc.; Raymond Abdo, DPM – St. Louis Foot & Ankle; Sebastian Cruz-Schiavone, MD – Adamant Medical Group; Nathan Krehbiel, BSN, RN – MolecuLight, Inc.; Audrey Moyer-Harris, BSN, RN, MBA, CWS – MolecuLight, Inc.; Alyssa McAtee, PT, DPT – MolecuLight, Inc.; Isabel Baker, BSN, RN, WCC, OMS – MolecuLight, Inc.; Micaela Gray, MSc – MolecuLight, Inc.; Monique Rennie, PhD – MolecuLight, Inc.
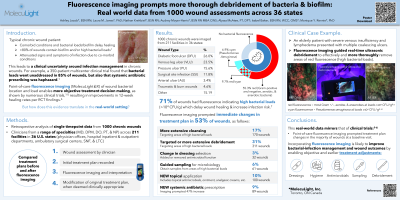
Introduction: The presence of high bacterial loads in chronic wounds increases the risk of complications, such as infection and hospitalization, and inhibits healing processes. Healing outcomes are shown to improve when more bacteria are removed through hygiene, biofilm disruption, more frequent debridement, and more aggressive debridement methods. Point-of-care fluorescence (FL) imaging* information on wound bacterial location(s) and load can inform treatment decisions, including the need for more extensive or expansive debridement. This retrospective study evaluates the prevalence of elevated bacterial presence in wounds across 36 states and the impact of that location and load information on treatment plans in a real-world setting.
Methods: This retrospective analysis evaluated single time-point treatment decisions from 1000 chronic wounds (DFUs, VLUs, PUs, surgical wounds, burns, and others) assessed by clinicians at 211 facilities across 36 US states. No exclusion criteria were applied. Clinicians proposed treatment plans for each wound before and after FL-imaging were recorded, including clinical signs and symptoms of infection (CSS), FL-imaging findings, and any treatment plan changes.
Results: FL signals indicating elevated bacterial loads were observed in 701 wounds (70.8%), but CSS were present in only 293 (29.6%). Post FL-imaging, treatment plans changed in 528 (53.3%) wounds: change in dressing selection (3.2%), more extensive hygiene (17.2%) or debridement (18.7%), FL-targeted debridement (17.2%), FL-guided sampling for microbiological analysis (6.2%), new topical therapies and systemic antibiotic prescriptions (10.1% and 9.0%, respectively).
Discussion: These real-world findings of asymptomatic bacterial load/biofilm prevalence, and of the frequent treatment plan changes post-imaging, are in keeping with clinical trial findings on this technology. These data, from a range of wound types, facilities, and clinician skill sets, suggest that point-of-care FL-imaging information improves bacterial-infection management.

.png)