(CR-054) A Prospective Multicenter Randomized Controlled Open-label Trial to Assess the Clinical Effectiveness of a Decellularized Full-thickness Placental Membrane in Patients with Diabetic Foot Ulcers: Preliminary Results
Introduction: Chronic wounds, such as diabetic foot ulcers (DFUs), impose substantial treatment and cost burdens on global healthcare systems, representing an estimated 1 to 4% of total healthcare spending in developed countries.1 Allografts derived from the placental membrane obtained from consenting live-birth donors have emerged as an important treatment option for such chronic wounds, but often have poor handling characteristics.2 To create a thick, easy-to-handle placental allograft while retaining growth factors, the first minimally manipulated, intact full-thickness placental membrane (FTPM) to include a decellularized trophoblast layer was developed. Here, we present preliminary results from an ongoing multicenter study that assesses the clinical effectiveness of this FTPM in treating DFUs.
Methods: Following screening and 30-day run-in to verify wound status and stability, up to 120 patients are randomized at a 1:1 ratio to receive either FTPM or conventional care (CC; ie, moist-wound therapy). Following baseline evaluation and treatment, weekly evaluation/treatments occur for up to 12 weeks or until 100% re-epithelialization is observed and verified for 2 weeks (defined as healed). In the FTPM group, investigators may perform additional applications in Weeks 1 through 11. The primary endpoint is the proportion of patients healed by Week 12 in each group. Secondary endpoints include mean percent wound closure at Weeks 1 through 12 and mean number of FTPM applications.
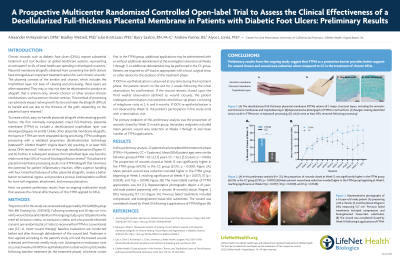
Results: In this preliminary analysis, 25 patients had completed the treatment phase (FTPM = 14 patients, CC = 11 patients). Mean (SEM) patient ages were similar between groups (FTPM = 62.3 [2.7] years, CC = 56.2 [3.3] years; p = 0.1636). The proportion of patients healed at Week 12 was significantly higher in the FTPM group (64.3%) vs the CC group (27.3%; p < 0.0001). Percent wound closure trended higher in the FTPM group beginning at Week 3, reaching significance at Weeks 9 (p = 0.0157), 10 (p = 0.0039), and 11 (p = 0.0348). The mean (SEM) number of FTPM applications was 8.4 (1.1).
Discussion: Preliminary results from this ongoing study suggest that FTPM demonstrates superior rates of healing and wound area reduction when compared to CC in the treatment of chronic DFUs.

.png)