(CS-042) Management of intravenous drug abuse (IVDA) soft tissue injuries with the continuum of negative pressure wound therapy
Friday, April 28, 2023
7:15 PM - 8:30 PM East Coast USA Time
Amir Behnam, MD – Chief of Plastic Surgery, Reding Hospital
Introduction: Soft tissue injuries (STI) resultant of intravenous drug abuse (IVDA) are rising nationwide. New varieties of drugs with toxic adulterants have led to necrotizing skin ulcerations/injuries. 1 One such adulterant, xylazine (ana2-adrenoreceptor agonist), is not FDA approved in humans but has surgical applications in veterinarian medicine as a sedative-hypnotic, anesthetic, muscle relaxant, and analgesic. 1,2 Xylazine, known colloquially as “Tranq,” has been used to cut opioid drugs for illicit use. 1,3 Given the proximity of a Level 1 Trauma Center in eastern Pennsylvania to the Tranq epicenter in Philadelphia, our wound care team has encountered multiple IVDA-associated injuries. 1,4 Persons who inject drugs (PWID) that present with skin ulcerations are treated with surgical interventions but are often left with considerable tissue deficits. 1,4,5
Methods: : Patients with IVDA-induced STIs were treated via fasciotomy and/or excisional debridement and negative pressure wound therapy (NPWT*). Where applicable, different NPWT platforms were enlisted to either cleanse (NPWT with instillation and dwell; NPWTi-d†) the wounds or to help bolster a skin graft. Additional surgeries were performed, as needed, to apply cellular tissue product or split-thickness skin grafts (STSG).
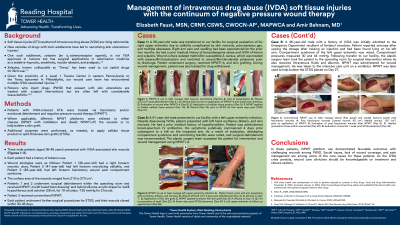
Results: Three male patients (aged 36-46 years) presented with IVDA-associated skin wounds. Each patient has history of smoking tobacco. Wound etiologies were as follows: Patient 1 (36-year-old) had a right forearm necrotic ulcer, Patient 2 (41-year-old) had left forearm necrotizing cellulitis, and Patient 3 (46-year-old patient) had left forearm fasciotomy wound post compartment syndrome. The surface area of the wounds ranged from 210-273 cm2. Patients 1 and 2 underwent surgical debridement within the operating room and received NPWTi-d with fused foam dressing‡ and hybrid silicone-acrylic drape§ to instill hypochlorous acid solution (28 mL for 10 minutes; -125 mmHg for 2 hours). Patient 3 received conventional NPWT. Each patient underwent further surgical procedures for STSG, and their wounds closed within 30-38 days.
Discussion: In these patients, NPWT platform use demonstrated favorable outcomes with challenging wounds among PWID. Social issues, lack of wound coverage, and pain management are among some of the care issues for these patients. As the IVDA crisis persists, wound care clinicians should be knowledgeable on treatment and closure options.

.png)