(CS-077) Allograft Adipose Matrix Injection for the Treatment of Fat Pad Atrophy with Recalcitrant Ulceration- A Case Report
Friday, April 28, 2023
7:15 PM - 8:30 PM East Coast USA Time
Shuja Abbas, DPM; Ahmad Saad, MS4; Lady Paula DeJesus, DPM
Introduction: Pedal fat pad grafting is a minimally invasive therapeutic option for treating pedal fat pad atrophy and plantar ulcerations. The loss of tissue between the bone and the skin can lead to chronic non-healing ulcers. This study describes the novel technique of allograft adipose matrix (AAM) to increase plantar fat pad thickness, therefore avoiding chronic ulcerations that can ultimately lead to infection and loss of limb/life.
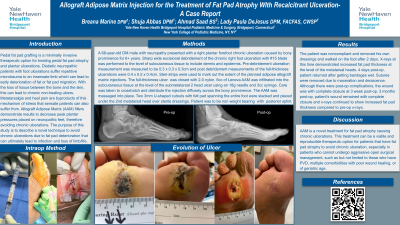
Methods: A 68-year-old DM male with neuropathy and a right plantar forefoot chronic (6+ years) ulceration caused by bony prominence. Excisional debridement of the chronic right foot ulceration sub metatarsal 2 head with #15 blade was performed to the level of subcutaneous tissue with pre and post debridement measurements. Steri-strips were used to mark out the extent of the planned AAM injections. 6cc of AAM* was infiltrated into the foot from the distal-medial aspect of the ulceration site. Immediately after infiltration, minimal AAM* leaked out of the ulceration. The decision was made to suture the full-thickness ulcer closed with 2-0 nylon. The AAM* was infiltrated into the subcutaneous tissue at the level of the sub metatarsal 2 head ulcer. Care was taken to crosshatch and distribute the injection diffusely across the bony prominence. After accounting for some wasted material and leaked adipose tissue, approximately 3-4cc total of the AAM* injectable filler were infiltrated into the ulceration and massaged into place.
The surgical site was dressed with sterile dressings. Two 3mm U-shaped felt cutouts overlying the second metatarsal head were placed over dressings. Webril & a posterior splint was applied. Strict non-weight bearing instructions given.
Results: Patient followed up 2 days post-op, as they had removed their dressings and been weight bearing. X-rays demonstrated increased fat pad thickness at the level of the metatarsal heads. 4 days post-op patient returned to clinic after soaking bandages. Surgical site was macerated and sutures were removed. Despite complications, the wound had complete closure at 3 weeks post-op. 3 months post-op patient’s wound remained fully closed and x-rays continued to show increased fat pad thickness compared to pre-op x-rays.
Discussion: AAM grafting is a novel treatment for fat pad atrophy causing chronic ulcerations. This treatment can be a viable and reproducible therapeutic option for patients that have fat pad atrophy to avoid chronic ulceration, especially in patients who cannot undergo open surgical management due to comorbidities (PVD, poor wound healing, geriatric age, etc.).

.png)