(CS-115) Novel Extended Wear Powder Dressing Used in Patient with Large Surgical Wound s/p Spinal Epidural Abscess Evacuation and Potential Risk of Autonomic Dysreflexia
Friday, April 28, 2023
7:15 PM - 8:30 PM East Coast USA Time
Michael Bellew, MD; Amay Parikh, MD
Introduction: The incidence of spinal epidural abscess has increased in the United States over the last 40 years, largely due to an aging population, increased number of spinal procedures (including epidural anesthesia), intravenous (IV) drug abuse, and increased number of compromised immune system conditions (e.g., diabetes mellitus, AIDS, cancer, etc.).1 Surgical decompression remains the mainstay treatment1. Postoperatively, these surgical wounds can be extremely difficult to manage due to concern for autonomic dysreflexia (AD) given spinal cord involvement.2
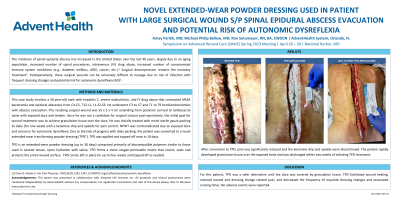
Methods: This case study involves a 56-year-old male with hepatitis C, severe malnutrition, and IV drug use found to have MSSA bacteremia, and epidural abscesses from C4-C5, T12-L1, L1-S2-S3, who underwent C3 to C7, and T1 to T9 hemilaminectomies with abscess evacuation. Surgical wound was 55 x 5 x 4 cm extending from posterior cervical to lumbosacral spine with exposed dura and tendon. Because he was not a candidate for surgical closure post-operatively, the initial goal was to achieve granulation tissue over the dura. He was initially treated with packing twice daily (for one week), and negative pressure wound therapy (NPWT) twice a week (requiring 2 hours of WOC time each change), with a ketamine drip and opioids for pain control. However, because of difficulty sealing NPWT over exposed bone and tendon, and concern for AD, NPWT was discontinued after a week, and he was converted to a novel transforming powder dressing (TPD). TPD is an extended wear powder dressing comprised primarily of biocompatible polymers used in contact lenses. Upon hydration with saline, TPD transforms into a moist oxygen-permeable matrix that covers, seals and protects the entire wound surface. TPD was applied to this patient twice over 10 days.
Results: Once converted to TPD, pain was significantly reduced, and the ketamine drip and opioids were discontinued. He developed granulation tissue over the exposed bone and was able to be discharged within 2 weeks of initiating TPD treatment.
Discussion: For this patient, TPD was a safer alternative than NPWT until dura was covered by granulation tissue. TPD facilitated wound healing, reduced wound related pain, and decreased frequency of dressing changes and nursing time. No adverse events were reported.

.png)