(CS-142) Intact Fish Skin Xenograft: A novel concept for treating large soft tissue defects after necrotizing soft tissue infection of the back
Friday, April 28, 2023
7:15 PM - 8:30 PM East Coast USA Time
Introduction: Necrotizing fasciitis (NF) is defined as a severe and lethal bacterial infection that occurs with a rapid onset resulting in extended soft tissue and fascial necrosis with relative sparing of skin and muscle. Here, we report the case of a 64-year-old African- American female with diabetes mellitus type 2 who was initially treated at a hospital for a back wound, developed NF, diverted and transferred to our burn unit with involvement extending from bilateral upper back to the bilateral gluteal area.
Objective: To explore the surgical strategy of acellular fish skin in wound bed restoration in a diabetic patient diagnosed with extensive necrotizing fasciitis.
Methods: Total body surface area posterior back was approximately 18%. Early debridement on day 2 of admission with application of negative pressure wound vac therapy for 3 days to stimulate a granulating wound bed. Subsequent surgical debridement ensued with the first application of intact fish skin graft. We used a 3 layer “stacked” method of intact fish skin graft to ensure adequate coverage and to minimize tissue deficits. A “Rolled” configuration of the fish graft was placed between wound bed and skin flaps located superior, lateral and inferior edge. On hospital day # 45, a split thickness skin graft, meshed 4:1 was performed along with autologous skin cell suspension. This was buttressed in place with burn mesh gauze. On hospital day 63, split thickness skin graft was meshed at 2:1 was placed on the sacrum.
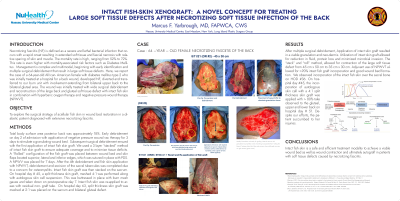
Results: Utilization of intact skin graft allowed for reduction in fluid, protein loss and minimized microbial invasion. The “stack” and “roll” method, allowed for contraction of the large soft tissue defect from 45 cm x 50 cm to 35 cm x 30 cm. Adjuvant use of NPWVT allowed for >90% intact fish graft incorporation and good wound bed formation. We observed incorporation of the intact fish skin over the sacral bone on HOD #36. On hospital day #45, the incorporation of autologous skin cell with a 4:1 split thickness skin graft was applied with > 80% take observed to the gluteal, upper and lower back on hospital day # 51. Despite our efforts, the patient succumbed to her injuries.
Discussion: Intact fish skin is a safe and efficient treatment modality to achieve a viable wound bed as well as wound contraction and ultimately autograft in patients with soft tissue defects caused by necrotizing fasciitis.

.png)