(DLS-026) Limb salvage of the lower extremity following acute traumatic compartment syndrome
Friday, April 28, 2023
7:15 PM - 8:30 PM East Coast USA Time
Genise Kennedy, DPM – Resident physician, Lourdes Hospital; Ian VanderGulik, DPM – Resident physician, Maryland Veterans Affairs Health Care System/Sinai Hospital of Baltimore; Nhi Le, DPM – Resident physician, Lourdes Hospital; Christopher Bibbo, DO/DPM, FACS, FAAOS, FACFAS – Head of Foot and Ankle Surgery, International Center for Limb Lengthening Assistant Director, Foot and Ankle Deformity Correction and Orthoplastics Fellowship Foot & Ankle Surgery, Plastic Reconstructive & Microsurgery, Peripheral Nerve Surgery, Limb Salvage, Deformity Correction, Orthopedic Trauma, Sinai Hospital of Baltimore
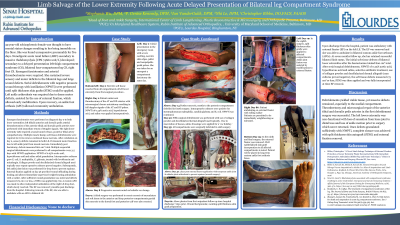
Introduction: 39 year-old schizophrenic female was found unresponsive presumably for five days. Nonoliguric acute renal failure (ARF) secondary to massive rhabdomyolysis [CPK 74660 unit/L] correlated with diagnoses of left thigh compartment syndrome (CS), bilateral four-compartment leg CS, right foot CS requiring emergent fasciotomies. She sustained severe sensory and motor deficits to the bilateral legs and large wound defects. Serial debridements with negative pressure wound therapy with instillation (NPWTi) were performed until split thickness skin grafts (STSG) could be applied. External fixation (EF) assisted left ankle arthrodesis. With an ankle foot orthosis (AFO), she could ambulate.
Methods: Emergent fasciotomies performed along with left tibialis anterior and dorsalis pedis arterial thrombectomies; right lower extremity (LE) required tarsal tunnel release and posterior tibial artery sympathectomy, six subsequent surgical debridements. NPWTi of 0.25% acetic acid, hypochlorous acid and saline aided granulation. Collagen powder and decellularized dermal allograft used topically once repeat operative cultures proved negative. Subsequently, left ankle joint fusion was performed to prevent equinus. EF provided wound offloading during healing and immediate weight-bearing ambulation with physical therapy for three months duration. Sufficient wound granulation on HD #79, STSG was applied. An AFO was used to support the right LE.
Results: Positive dopplerable signals after thrombectomy and microsurgical repair of the anterior tibial and dorsalis pedis arteries. After extubation on HD#2, sensory deficits remained to both LE. Permanent motor function loss to left ankle joint from muscle necrosis. Immediately post fasciotomy, defects measured 800 cm2 total. Once serial debridements yielded viable tissues with defects measuring 75 cm2 or less, STSG was applied. Cultures grew E. coli, S. maltophilia, C. glabrata, treated with levofloxacin and micafungin. EF removal three months later. She ambulated with a walker and bilateral AFOs two weeks postdischarge.
Discussion: Acute CS has rarely been reported associated with acute rhabdomyolysis. After emergent fasciotomies and intensive management, above knee amputation occurred in one case1. Our patient had a chronic DVT to LE resulting in CS with acute rhabdomyolysis and ARF, reversed after temporary dialysis. This was a successful limb salvage due to arterial reperfusion which is pertinent in most CS cases2. Some literature states delayed fasciotomy results in higher risk of amputation, time to fasciotomy is not associated with limb amputation in CS3. In our case, the patient was five days out. However, amputation was avoided due to multiple salvage attempts with serial debridement, NWPTi, and sequential EF application.

.png)