(CS-125) Clinical management of non-uremic calcific arteriolopathy
Friday, April 28, 2023
7:15 PM - 8:30 PM East Coast USA Time
Introduction: Calcific arteriolopathy, formally known as calciphylaxis, results in calcium deposition in the arteries and arterioles of the soft tissues leading to painful ischemia, thrombosis, and cutaneous necrosis. Calcific arteriolopathy commonly associated with end stage renal disease (ESRD) and hemodialysis patients, but it can also occur outside of ESRD. This is then known as non-uremic calcific arteriolopathy (NUC). NUC has a high associated mortality rate of 52%, which is primarily due to sepsis (50%). Biopsy of lesions is considered the primary diagnostic. Therapeutic interventions have historically been targeted towards the presumed etiology of uremic calcific arteriolopathy including sodium thiosulfate administration. These interventions have less available evidence of clinical success when used in NUC.
Methods: The clinical presentation and successful treatment of 3 cases of NUC treated at a southeastern Wisconsin community hospital outpatient department is discussed herein.
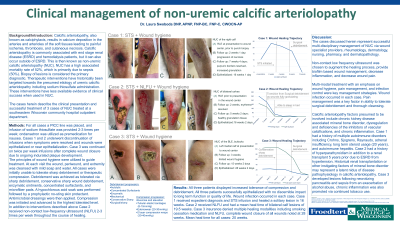
For all three cases a PICC line was placed, and infusion of sodium thiosulfate was provided with premedication for nausea with ondansetron. Infusions were discontinued when symptoms were resolved, wounds were epithelialized, or near epithelialization.
At each visit the wound, periwound, and extremity was cleansed with mild soap and water. All cases were initially unable to tolerate sharp debridement or therapeutic compression. Debridement was achieved as tolerated via sharp debridement, enzymatic ointments, concentrated surfactants, and microfiber pads. A hypochlorous acid soak was performed followed by a no-sting skin protectant. Antimicrobial dressings were then applied. Compression was initiated and advanced to the highest tolerated level.
In addition to interventions described above Case 1 and Case 2 received non-contact low-frequency ultrasound (NLFU). NLFU was provided 2-3 times per week throughout the course of healing.
Results: All three patients displayed increased tolerance of compression and debridement. Wound infection occurred in each case, and was quickly identified and treated. Pain management was a key factor in ability to tolerate surgical debridement and allow for thorough cleansing.
All three patients successfully epithelialized with no discernible impact to long term function or quality of life.
Discussion: The cases discussed herein represent successful multi-disciplinary management of NUC via wound specialist providers, rheumatology, dermatology, nursing, pharmacy, and dermatopathology. Non-contact low frequency ultrasound was chosen to augment the healing process, provide biofilm based wound management, decrease inflammation, and decrease wound pain. Multi-modal treatment with an emphasis on wound hygiene, pain management, and infection control were key management strategies.

.png)